Introduction
This lens fit appears like a complex case, with at least three different factors playing a role. But by ‘simply’ applying a basic set of rules, this case report shows what a difference an Eye Care Professional (ECP) can make in people’s lives. First, by assessing whether an eye is ‘standard’ or not, the ECP can determine whether one of our standard off-the-shelf lenses would be the best lens option, with many benefits including material choice, pricing and – especially – frequency of replacement. ‘Simply’ because the ocular surface is steep and outside the range of the normal eye, choosing a ‘steep lens’ based on sagittal height can make the difference. In addition, there is the challenge (or not) of the lens prescription and material considerations. Not that complicated at all, and, in fact, without a steep learning curve.
Subjective
Tessa came to our practice right in the heart of Amsterdam in the Netherlands. Her prescription is out-of-standard. The feasibility of a standard monthly lens is explored but was questioned. With her high hyperopic prescription, the cosmetic and visual effects of contact lenses over glasses should not be ignored (large visible eyes, aberrations, magnification and sub-optimal visual acuity with glasses).
In the past, she had tried different lens types, with a long track record including, but not limited to Durasoft 3 (Wesley Jessen), Unilab 42C toric (Taiwan) and StabMax (MicroLens). Reproducibility used to be a major problem in the past with custom-made lenses; a problem that has been mostly relegated with current manufacturing techniques. The patient history did not reveal any special or specific considerations or limitations for fitting with a soft lens, other than that she reported having mild dry eyes.
Objective
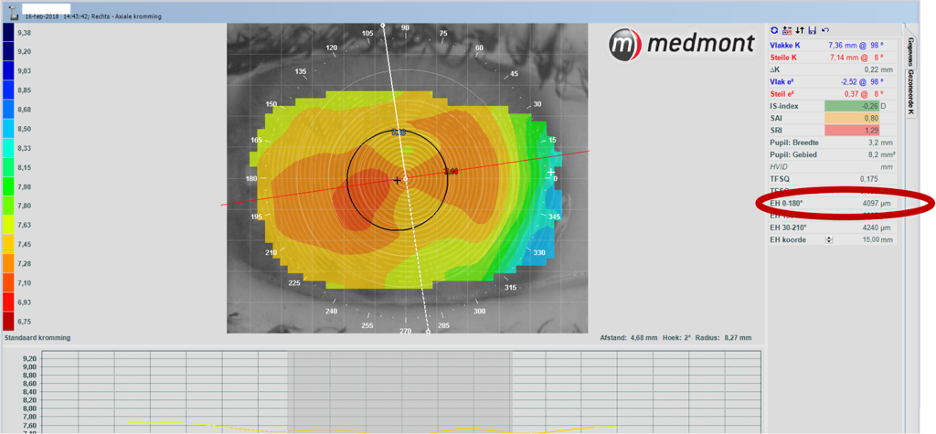
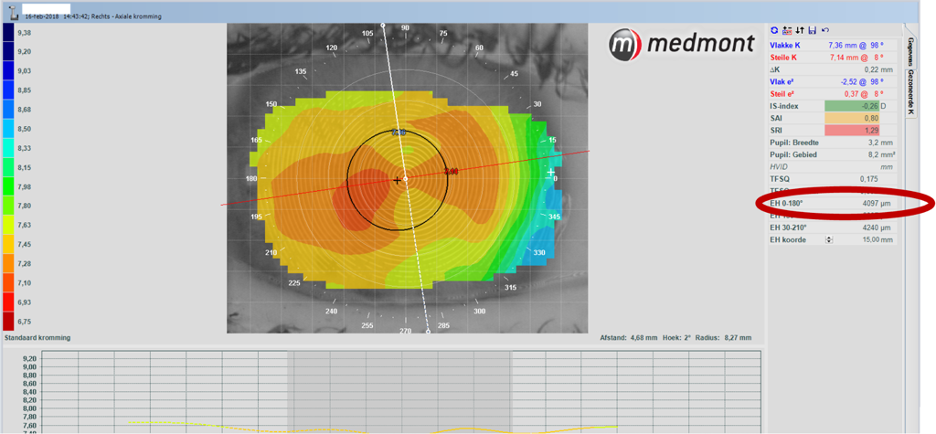
General slit lamp examination revealed no abnormalities. Refraction of the patient (in this case report we focus on her right eye) came down to: S+4.75=C -5.00 x 90°. Her sim-K values are 7.36/7.14, with eccentricities reported in four different quadrants as: 0.45 superior, 0.71 nasal, 0.58 inferior and 0.35 temporal.
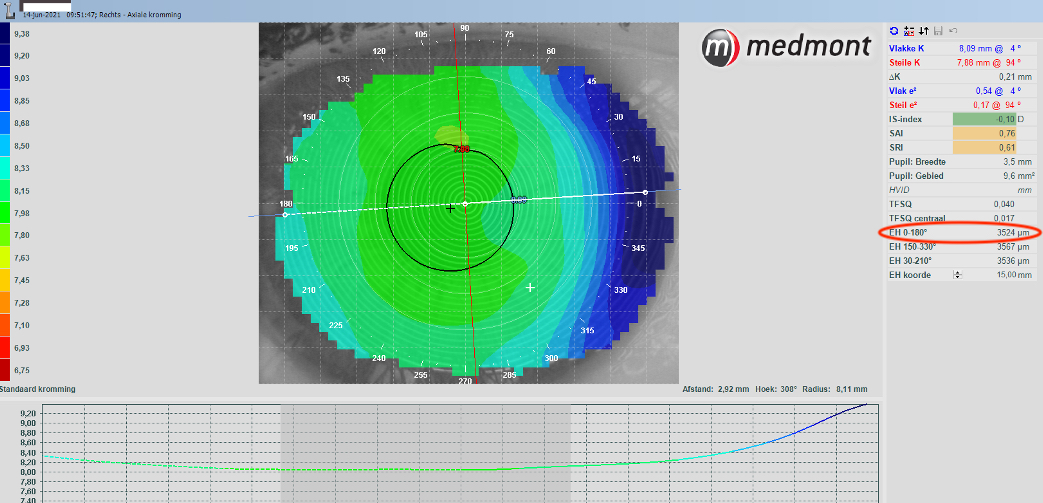
In our contact lens practice, special emphasis is on the shape of the anterior ocular surface. We use a Medmont corneal topographer with a special tool: the E-H software*. Based on the overall corneal topography using that instrument, the peripheral corneal angle measured with the corneal topographer and using the sagittal height calculator – the overall sagittal height of the ocular surface (OC-SAG) over 15mm can be estimated, typically the horizontal meridian values are used.
Assessment
In this case, the E-H 0-180° value was 4097µm. This is well beyond the OC-SAG of the average eye (which is estimated to be in the 3750µm range). In fact, it falls outside the one-standard deviation range (between 3550-3950µm). The fact that this eye falls on the right side of the normal distribution bell curve and even outside the 1-SD range (accountable for 66.7% of all eyes) – indicates that this is an out-of-standard steep eye. Based on keratometry values alone (7.36/7.14), and even in combination with the eccentricity values this time (0.53, which is standard), it is not easy to judge that in the same way. Her corneal diameter (white-to-white) measured with the Medmont was 11.2mm which is slightly smaller than normal.
In addition, the prescription’s astigmatism does not match the corneal astigmatism data (the difference in central keratometry values is only 0.22mm, which represents roughly an astigmatism of 1 diopter, while the refraction indicates 5 diopters of astigmatism). The refractive (rest) cylinder must therefore come from the crystalline lens or another internal astigmatism in the eye.
Plan
For this patient, it was decided not to start with standard lenses but go directly to an out-of-standard lens – to satisfy both the refractive and ocular surface shape peculiarities of this patient’s eye.
With any toric lens, but certainly, with an astigmatism of this magnitude, good stabilization of the lens on-eye is crucial. Fitting a toric lens is not a disadvantage, in this case, though – but rather an advantage. Since most soft toric lenses have their toricity based on the inside of the lens – this can help stabilization with higher cylindrical values. In other words: a 5D cylinder stabilizes better most probably than a 0.75D cylinder.
In addition, ECPs can choose to fit a slightly steeper lens, to aid stability of the lens on-eye and/or to choose a larger diameter. But for this, it is important to know how steep the eye is. This cannot be judged by central keratometry values and/or eccentricity alone, as this case shows. The eye is exceptionally steep, and to create stability an even steeper lens would be needed. A 7.70 lens was selected in the end, with a lens diameter that is not larger than normal (because of her corneal diameter). But the result is a lens with an out-of-standard high sagittal height value. Using sagittal height values, in this case, makes more sense than using base curve values.
A Gentle 80 Toric (Mark’Ennovy, Madrid ES) was used in this case: BC 7.70 S+5.00=C -5.00 x 95° Æ14.0. This is an 80% hydrogel lathe-cut soft lens for monthly replacement. The lens with these parameters is calculated to have a CL-SAG of 4100µm. This material, a non-silicone hydrogel (SH) material was preferred over the silicone hydrogel lathe-cut soft lens variant (Saphir Rx ) for monthly replacement, because of wettability issues with the SH lens material.
In Summary
It can be determined that there are 3 categories of soft lenses:
(1) off-the-rack standard soft lenses;
(2) out-of-standard lenses with extended parameters;
(3) custom-made individually designed lenses.
For patients like this, the number 1 category is out of range.
First: the refraction is out of the standard lens’ parameter range. In these cases, category 2 lenses can be a huge asset and can prevent drop-out of lens wear. In this case, it was not just a special optical case, but also an ocular surface shape outlier: an exceptionally ‘steep’ eye that desired a special design with a higher-than-normal CL-SAG. Both optically, and in terms of lens comfort, this lens performs better than previous lenses. As a third variable, the silicone hydrogel lenses originally selected did not provide the desired wettability. Switching to a non-SH solved this problem. Careful checks for hypoxic signs on the eye are monitored. But having the option to switch material, whilst staying in the same lens design – can be a huge plus for ECPs when fitting soft specialty lenses.
This case shows that, albeit ‘complex’ at first, applying simple rules towards (1) eye shape, (2) prescription and (3) material properties can make a big difference in contact lens practice.
*the E-H tool in the Medmont topographer can be added simply, using the manufacturers guidelines.
This case study is part of a series focusing on speciality soft lens fitting. Stay tuned for the next installment coming soon. Special thanks to Eef van der Worp for bringing this series together.